¶ 1 Leave a comment on paragraph 1 0 Welcome. Please read the instructions for reviewing before commenting. We ask contributors to be generous when thinking along with our pieces and to keep in mind that the final chapters are intended to be short essays. Visit matteringpress.org for more information on its other books. Readers might also want to have a look at this resource created by one of the book’s editors, Emily Yates-Doerr, which catalogues key Open Access anthropology publications.
¶ 2 Leave a comment on paragraph 2 0 By Susan Reynolds Whyte
¶ 3 Leave a comment on paragraph 3 0 There was a small glitch when our book Second Chances was almost ready to go to press. It was a layout problem. The Table of Contents was congested with too many chapters, too many vignettes, and too many authors.[i] We had to drop the authors’ names and in the end, for technical reasons, the good people at Duke set the vignettes instead of the chapter titles in bold. The Table of Contents that went to press gives the impression that we have made a casebook—a set of descriptive instances of individual people who survived AIDS when antiretroviral medicines became widely accessible. The problem that remained was not a layout problem but an authorial problem: the cases were highlighted and we who had authored them were in shadow.
¶ 4
Leave a comment on paragraph 4 0
¶ 5 Leave a comment on paragraph 5 1 ‘We’ is a definitely plural pronoun. We were eight people,[ii] four from Denmark and four from Uganda, who did a study and wrote a book about it. All eight of us were authors, but our book is neither a monograph nor an edited volume in the conventional sense. We call it a polygraph. It resembles a lie detector—not because it reports a singular truth or discerns untruths, but because it marks vital processes simultaneously at different points in a social body. And it is based on polygraphy in the old sense of copious writing—piles of handwritten fieldnotes transcribed to electronic text.
¶ 6 Leave a comment on paragraph 6 0 We had worked together for years before we decided to systematically document a dramatic turn in Ugandan history: the ‘rollout’ of free antiretroviral medicines. In one way or another, we had all been touched by the AIDS epidemic—by the feelings of helplessness and injustice as people we cared about suffered and died while medicine was saving lives in richer parts of the world. When the antiretrovirals (the ARVs) were finally provided for free around 2005, a whole generation of people who expected to die of AIDS got a second chance to live. We wanted to write about those people.
¶ 7 Leave a comment on paragraph 7 0 We never doubted that the way to do it was to start with life stories. It seemed obvious because HIV had already become a narrativized condition. Positive people were encouraged to open up, to testify about their experiences to their peers and their treatment providers. News media were eager for the existential dramas of sex, life and death. Organizations supplying the medicines needed the personal accounts to justify the enormous expenses being poured into the effort. Public health researchers, as well as social scientists, found that experience-near descriptions made their analyses credible.
¶ 8 Leave a comment on paragraph 8 0 Case stories also seemed evident as an anthropological method. We were Africanists for whom the extended case and the situational analysis of the Manchester School were exemplary. We had seen the power of carefully unfolding a situation, progressively contextualizing it so as to portray a political economy or a broader pattern. It was a way to do ethnography.
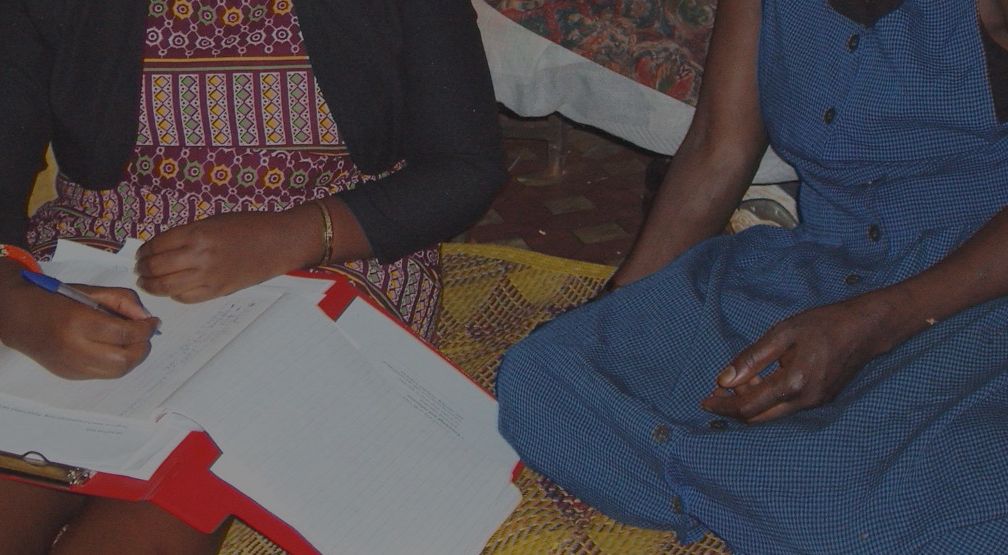
¶ 9 Leave a comment on paragraph 9 1 The narrative possibilities pulled us as well. We saw the chronological potential in retrospective life histories combined with prospective following along through visits over a period of time. Stories of individuals would allow us to make connections over time, to see how one thing led to another, and more importantly, to listen to how our interlocutors knitted threads together or dropped stitches. So it was with the woman we call Jackie, whom our colleague David visited over a year and a half. In a strikingly frank manner, she confided her experiences and the surprising turns that her life took.
¶ 10 Leave a comment on paragraph 10 0 Early in their acquaintance Jackie told David how unhappy she was that Joseph, the father of her younger children, kept their relationship a secret. He refused to introduce Jackie to his parents, thus declining her recognition as a wife and denying their children acknowledgment as grandchildren. Although he clandestinely paid for the treatment of their HIV positive child, he would not publicly admit that he was the father. She was torn, wanting to leave him, but reluctant to forego the support he was giving her. On one occasion, Jackie even asked David for advice about what to do.
¶ 11 Leave a comment on paragraph 11 0 Finally she decided to make a break; she got ‘saved’ in a Pentecostal church and began saying that Joseph had demons, and that they were committing the sin of adultery. Indeed, Joseph was formally married; his first wife had made a point of asking Jackie if she knew why all of the children of this first marriage had died, implying that Joseph was HIV positive. At one visit, David found that Jackie had moved out of the rooms she shared with Joseph. But the split did not last long; she remarked that perhaps it was God’s plan that she should stay with Joseph. Still they quarreled regularly; she insinuated to him that he was the one who had infected her, even though she had earlier told David about the HIV diagnosis of her first partner, father of her eldest child.
¶ 12 Leave a comment on paragraph 12 0 At the last visit, she gave David the startling news that Joseph had died. Hoping at last to gain recognition from his family, she gathered the children and took them to the funeral where they could be presented as his only living heirs. Surprisingly, however, three other women showed up with children who all claimed Joseph as their father. His family knew nothing of these women either, but said they were prepared to provide support for all of his children. Thus it was only upon his death that Joseph’s children gained paternal grandparents.
¶ 13 Leave a comment on paragraph 13 0 There were so many stories as fascinating as Jackie’s. We could have concentrated our efforts on fewer. But we wanted diversity, which we felt was often lacking in the studies we had read of AIDS patients. We wanted to talk to men and women, poor and better off, rural and urban, and clients of different treatment programs, including some who had tried to pay for their treatment in the days before it was available for free.
¶ 14 Leave a comment on paragraph 14 0 We contacted 48 people on antiretroviral therapy, through seven different treatment facilities, and asked them to tell us their life stories, not just their sickness stories. How did you grow up, what about your family, your work? From the beginning we tried to talk to people in their everyday settings, not at their places of treatment, a strategy that de-centered AIDS and brought out what people were making of their second chances. Among these 48, we identified 23 whom we visited seven more times. And here I should write ‘they’ instead of ‘we’, because the Ugandan members of our team did most of the talking and visiting. From Denmark we followed along, reading the notes as they ticked in on our computers. And whenever we were in Uganda, we went along on the visits. But by and large, it was David and Jenipher and Phoebe and Godfrey who got to know the individuals, homes, families and workplaces of the people who became our cases.
¶ 15
Leave a comment on paragraph 15 0

¶ 16 Leave a comment on paragraph 16 0 The visits and revisits developed differently. Some interlocutors became friends and the researchers got involved with their lives and problems as friends do. There were phone conversations and text messages between visits; the researchers got to know other members of the family and followed the tensions and détentes that are a normal part of family life. Other interlocutors remained acquaintances, who were welcoming on some occasions, and more reserved on others. There were dramatic moments, as when Jenipher arrived to find the man she was visiting in jail on allegations of stealing a sheep. And there were routine calls ‘just checking in’ when there was not much new to report.
¶ 17 Leave a comment on paragraph 17 0 When a year and a half had passed, the visits ended and we faced hundreds of pages of notes. Brainstorms and difficult choices and attempted divisions of responsibility followed, resolving into the plan that became Second Chances. The lives we had documented became cases as we began to treat them as source material—all 23 arranged neatly in ring binders ready to be mined for inspiration in writing the topical chapters that would compose the book. At this point they formed the stuff of classical extended cases, based on repeated conversations over more than a year and capturing multiple social positions and events. However our plan was not to work from case to case, but to abstract from this material in order to illuminate—but also to illustrate—our analytical points about generational consciousness, sociality and chanciness. Our extended cases provided both analytical insight and, when chopped into pieces, useful and hopefully ‘apt’ examples.
¶ 18 Leave a comment on paragraph 18 0 We also wanted to preserve some cases as longer texts that could convey to readers the individuality and diversity of the people whose lives were prolonged by ARVs. We hit on the idea of letting one case introduce each chapter—easy enough since the chapters themselves provided analytical discussions of everyday concerns like families, partners, food, work and so on. We selected cases for their evocation of the chapter topics, but they were always about all kinds of other themes as well. The longer texts provided singularities we sought to reason about, rather than mere material that could be assimilated to theories. Almost every case had a theme about children—children being the most important second chance for nearly everyone—but Jackie’s case showed with particular clarity how HIV played into the social recognition of children in this patrilineal society.
¶ 19 Leave a comment on paragraph 19 1 In many ways those cases are what capture readers, especially students, and allow them to see how we made the analyses that followed. One of the manuscript reviewers had cautioned us against presenting the material as ‘an array of cases laid out for the reader to inspect.’ In the end though, we did lay out an array and made a virtue of it. We found that the casebook format allowed us to discuss a corresponding assortment of analytical issues, while still ‘making a case’ in the sense of an overall argument about second chances. The polygraphic casebook also permitted us to capture what was essential about our enterprise: assembling evidence through multi-sighted investigation at several locations in the social body.
¶ 20
Leave a comment on paragraph 20 0
¶ 21 Leave a comment on paragraph 21 0 Susan Reynolds Whyte, Professor of Anthropology, University of Copenhagen, carries out research in East Africa on social efforts to secure well-being in the face of poverty, disease, conflict, and rapid change. For two decades she has worked with African colleagues on Enhancement of Research Capacity projects. She is the author of Questioning Misfortune: The Pragmatics of Uncertainty in Eastern Uganda and co-author of Social Lives of Medicines.
¶ 22 Leave a comment on paragraph 22 0 Notes
¶ 23
Leave a comment on paragraph 23 0
[i] 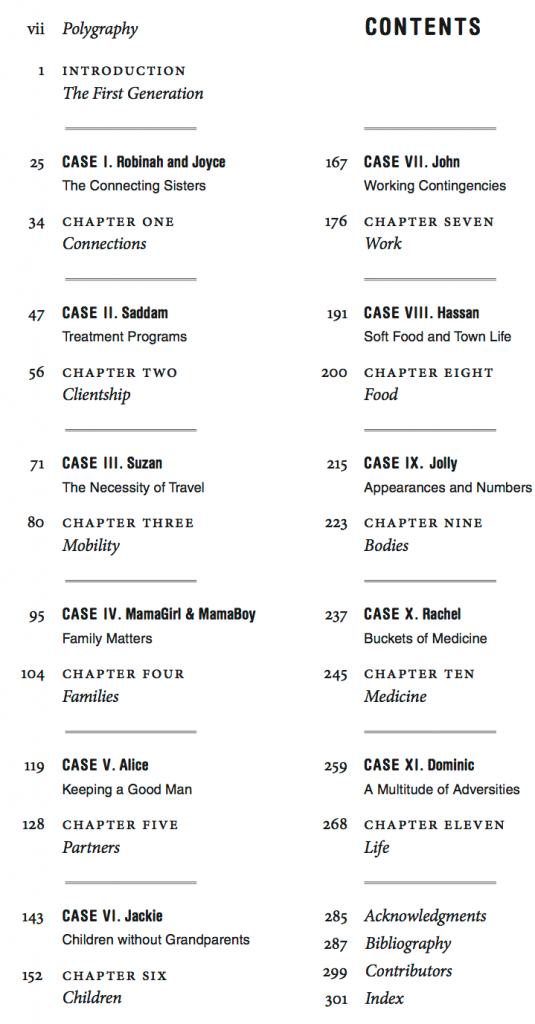
¶ 24 Leave a comment on paragraph 24 0 [ii] Phoebe Kajubi, David Kyaddondo, Lotte Meinert, Hanne O. Mogensen, Godfrey Etyang Siu, Jenipher Twebaze, Michael Whyte, and Susan Whyte
¶ 25 Leave a comment on paragraph 25 0 References
¶ 26 Leave a comment on paragraph 26 0 Whyte, Susan Reynolds (ed.) 2014. Surviving AIDS in Uganda. Durham: Duke University Press
This reminds me a bit of Dan Linger’s article in Ethos a few years ago “What does it mean to be someone else”. Linger makes a strong case for presenting many longer narratives with minimal interference, a resistance to an anthropology of “a single truth” as you put it so well.